The story of transplant medicine is one of the most beautiful and painful stories of modern medicine. In 1954, twin brothers were operated on in Boston, and one received a kidney from his brother. It was the first successful transplant ever, opening a new era where a failing organ could be replaced with a working one. Since then, millions of people have received second lives: kidneys, livers, hearts, lungs, pancreases, each taken from another person, dead or alive, and transplanted into a body that needed it.
But there is a structural problem in this story. Donors are a very limited resource, and there is a dramatic gap between supply and demand. In Canada alone, the organ waiting list today numbers over 4,400 people, and about 250 of them die each year before a suitable donor becomes available. In the US, the numbers are 25 times larger: over 100,000 waiting, and about 17 die every day. In Israel, over 1,200 people are on the list, and only about 450 transplants are performed per year.
On May 1, 2026, Hospital News published a report marking a turning point in this story. The world's first dedicated organ regeneration lab opened in Canada, a massive 12,000 square meter facility aimed at building whole organs from the patient's own stem cells, rather than waiting for a donor. If the approach works, it will turn the entire transplant paradigm on its head.
What is Organ Regeneration Anyway?
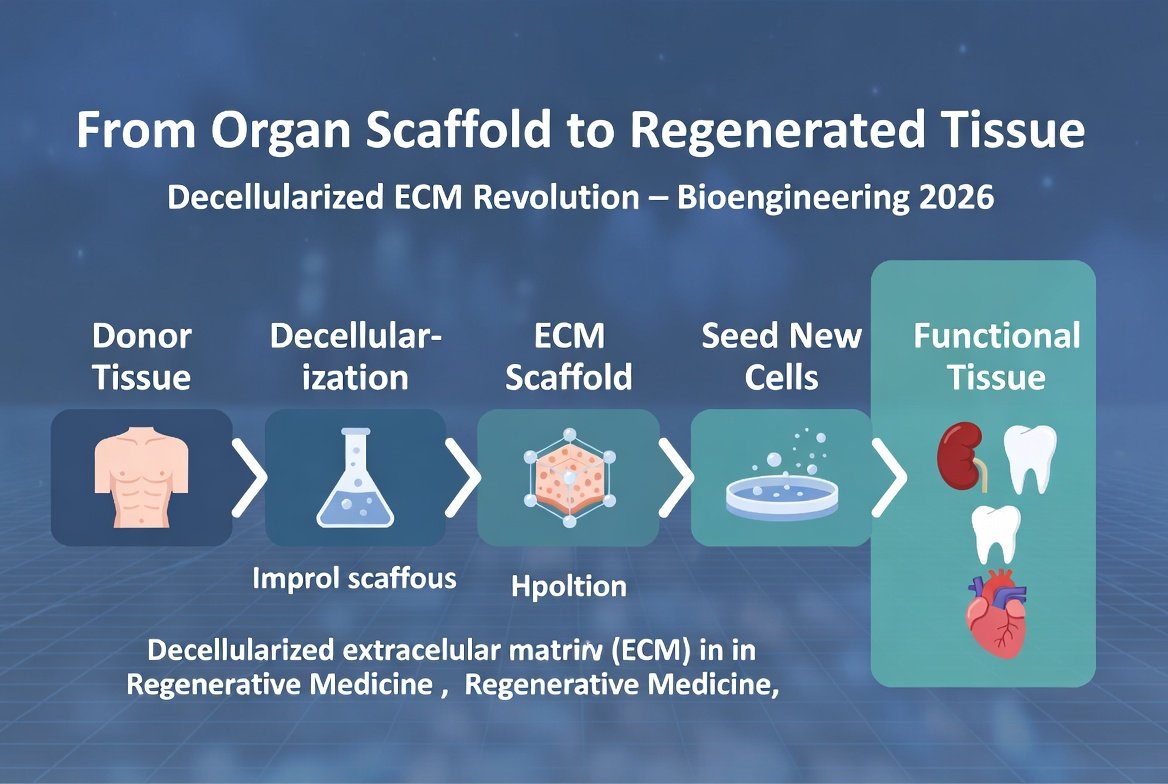
The term regenerative medicine describes a family of approaches aimed at growing, repairing, or replacing biological tissue using the body's own cells. Whole organ regeneration is the holy grail of the field, and is based on three core components:
- Extracellular matrix scaffold (ECM scaffold): The three-dimensional structure of an organ, including collagen, elastin, and laminin, without living cells. Imagine a house without tenants.
- Autologous stem cells: Stem cells derived from the patient themselves, usually iPSC stem cells reprogrammed from skin or blood cells.
- Bioreactor: A device that simulates physiological conditions in the human body, blood flow, pressure, oxygen, heat, and allows cells to divide and differentiate within the scaffold.
- Growth and differentiation factors: A series of proteins and signals that direct the cells to become heart, kidney, liver, or any needed organ tissue.
- Time: The process takes between 4 to 12 weeks for a whole organ, depending on its size and complexity.
The beauty of this approach is that the final organ immunologically is part of the patient. There is no need for immunosuppressive drugs that suppress the immune system for life, no risk of rejection, and no need for tissue matching. Additionally, there is no need for a donor, so there is no waiting list.
This approach is completely opposite to xenotransplantation (transplantation from animals, mainly genetically engineered pigs), which still requires immunosuppression and may cause cross-species infections. An organ from the patient's own cells is the perfect solution, if we can make it feasible on an industrial scale.
The Connection to Transplant Medicine: Bridging the Gap
To understand why this lab is groundbreaking, one must understand the gap between two worlds: classical transplant medicine and regenerative medicine.
Transplant medicine is built on transferring a living organ from one person to another. It works, it saves lives, but it depends on donors. In recent years, the demand for organs has grown significantly faster than supply, mainly because the population is aging and cases of organ failure are expanding. The average wait for a kidney in the US is 3-7 years, and about 13 people die every day on the waiting list for a kidney alone.
Regenerative medicine, on the other hand, is built on growing cells and tissues in the lab. It can produce infinite copies, it adapts itself to each patient, and it does not require a donor. The problem: until today, only flat and simple tissues have been successfully created in practice. Skin, cartilage, bladder, a few isolated cases of trachea. Complex organs like a heart or kidney were beyond technological capability.
The new Canadian lab attempts to break this barrier. It combines three technologies, each proven to work individually, but never combined on an organ scale: decellularization, repopulation with stem cells, and a physiological bioreactor. Whether they will indeed work together will be answered in the coming years.
Decellularization: Taking an Organ and Breaking Down Only the Cells
The central technique in the lab is decellularization, first developed by Doris Taylor in Minnesota in 2008. The idea is simple: take a donor organ (usually from a pig or a human that was not suitable for regular transplant), and wash it with detergent-like substances like SDS, which remove all cell membranes and DNA, but leave intact the extracellular matrix scaffold, that three-dimensional network of proteins that makes up the organ's structure.
The result is a transparent, white 'ghost organ', devoid of cells but with all the original geometry: blood vessels, kidney tubules, the essential chambers of the heart. It's like getting a ready-made house skeleton, full of floors and rooms, just without tenants.
The big advantage: this scaffold has already solved the hardest problem in tissue engineering, creating a three-dimensional blood vessel structure. You cannot grow a thick organ without blood supply at every point, and building a blood vessel network from scratch is nearly impossible. The natural scaffold preserves the blood vessels perfectly, and now only needs new cells to be introduced.
Repopulation with the Patient's Stem Cells
The second stage is recellularization. Autologous stem cells are taken, meaning cells derived from the patient themselves (usually iPSC, induced pluripotent stem cells, reprogrammed from skin or blood cells), and dispersed through the blood vessels of the scaffold. The cells find their way to their natural niches, attach to the scaffold, and begin to divide.
A series of growth factors and chemical signals directs their differentiation: heart muscle cells to the heart walls, endothelial cells to blood vessels, filtering cells to the kidney. Within 6-8 weeks in the bioreactor, the organ begins to function at a basic level: the heart starts to beat, the kidney starts to filter, the liver starts to produce albumin.
The Bioreactor: Imitating a Human Body
The bioreactor is an isolated chamber where the organ 'grows'. It must accurately simulate conditions inside the human body: a temperature of 37 degrees Celsius, oxygen and carbon dioxide at physiological concentrations, flow of culture medium through the blood vessels at the correct pressure, and even physical 'training'. A heart, for example, must 'exercise' against increasing pressure to develop strong muscle. A kidney needs to train against an osmotic gradient.
The bioreactors of the Canadian lab are the next generation: the size of a household refrigerator, equipped with dozens of sensors that measure the organ's function in real time, and connected to artificial intelligence that automatically adjusts conditions. Each bioreactor costs about 2.5 million dollars.
Current Evidence
Study 1: Rat Heart Revived from Minnesota (2008)
This was the first proof of concept. Doris Taylor's team decellularized a rat heart, repopulated it with new cardiomyocytes, and made it beat again in a bioreactor. The heart could produce 2% of the force of a natural heart, very little, but it beat. It was proof that the approach is possible.
The study was published in Nature Medicine and became one of the most cited in the field. Since then, hundreds of labs worldwide have replicated and advanced the technology. The 2008 heart beat for only a few minutes. Hearts from 2026, using the same approach, beat for entire weeks.
Study 2: Functional Pig Kidneys from Massachusetts (2022)
A team from Massachusetts General Hospital decellularized pig kidneys, repopulated them with human stem cells, and transplanted them into pigs. The kidneys filtered blood, produced urine, and maintained function for 30 days. While not enough to replace a real kidney, it proved the approach is scalable to human-sized organs.
Study 3: Human-Scale Pig Hearts from Texas (2024)
A lab at the Texas Heart Institute reconstructed a full pig heart, decellularized, repopulated with human iPSC cells, and grown in a bioreactor. The heart beat at a rate of 50-65 beats per minute, produced a cardiac output of 2.4 liters per minute (compared to 4-6 liters in a healthy human heart), and maintained function for three weeks. Not enough for human transplant, but closer than ever.
A critical detail: The heart was not 'rejected' by the immune system of experimental pigs, because the endothelium of the blood vessels was human. This is initial proof that the 'patient cells' strategy works immunologically.
Study 4: Miniature Liver Working for 7 Days from Japan (2025)
A team at Kyoto University built a palm-sized liver from human stem cells and transplanted it into a mouse with liver failure. The miniature liver produced albumin and broke down drugs for 7 days, increasing the survival of mice in the experimental group by 200%. It does not replace a full liver, but provides a 'bridge' for patients waiting for a transplant.
Study 5: 3D Bioprinting of Kidney Tissue (2025)
A lab at the Wake Forest Institute for Regenerative Medicine succeeded in printing a three-dimensional kidney structure using bioprinting of stem cells and matrix. The structure included functional filtering units (nephrons) that filtered 35% of what a healthy human kidney filters. The next step: enlarge the structure and connect to blood flow.
Study 6: The New Bioreactor System of the Canadian Lab
Initial publication from the Canadian lab. They developed an 'adaptive' bioreactor that uses artificial intelligence to adjust growth conditions in real time based on how the organ responds. In initial experiments on pig kidneys, organs grown in the new bioreactor showed 3 times better function than organs grown in static bioreactors.
What About Other Organs?
The Canadian lab is not focused on a single organ. It is designed to handle multiple organs, each with unique challenges:
- Kidneys: Target number 1. The longest waiting list, and a relatively simple structure. Expected to begin human trials in 2028.
- Heart: Target number 2. More complex, must beat and synchronize cellularly. Expected trials in 2030-2032.
- Liver: Target number 3. It is mainly a metabolic organ, but its geometry is complex with diverse liver cells. Expected in 2031-2033.
- Lungs: Long-term target. The alveolar structure is particularly delicate and hard to reconstruct. Expected in 2035 and beyond.
- Pancreas: Future target for type 1 diabetes patients, by growing new beta cells in a pancreatic environment.
- Trachea and larynx, smaller tissues like thyroid, adrenal glands, and lymph nodes are considered relatively 'easy wins' and will be attempted first.
In parallel, the lab will also develop partial tissues, not whole organs. Heart muscle patches after a heart attack, liver tissue to replace damaged liver, and kidney endothelial patches for partial damage repair. These will enter the clinic much before whole organs, perhaps as early as 2027.
Is This Realistic, or Is It Science Fiction?
The excitement is legitimate, but there are serious caveats to be aware of.
The Gap Between Model and Humans
All studies to date, even the most successful, were in animals. Humans are much more complex, live much longer, and require organs that function for decades, not weeks. It is possible that an approach that works for 3 weeks in a mouse will not hold up in a human for 30 years.
Ethics of Chimeric Organs
Some strategies involve using starting animals: for example, growing a human organ inside a genetically engineered pig. This raises deep ethical questions: is a pig with a human brain an animal or a half-human? Most groups, including the Canadian lab, avoid this approach and work with organ scaffolds only, without a living animal.
Astronomical Cost
Growing a personalized organ costs a fortune. At current values, growing a kidney from the patient's cells could cost 800,000-1.2 million dollars, more than a regular kidney transplant. Over time and with production scale-up, the price will drop, but it will take years. In Israel, the health basket certainly will not include this treatment in the coming decade.
Risk of Cancer from iPSC Cells
iPSC cells, cells reprogrammed to be pluripotent, carry a theoretical risk of cancer. If a cell does not fully differentiate in the organ and grows there with uncontrolled capacity, it could become a teratoma, a tumor containing multiple cell types. This risk is managed through strict quality control, but cannot be ignored.
Growth Time is a Clinical Barrier
Growing a kidney takes 6-10 weeks. A patient with acute kidney failure does not have this time. This approach is suitable for patients with chronic organ failure who have dialysis or bridging treatment, but not for acute patients. For acute cases, a donor kidney will remain the solution.
Realistic Timeline
If everything goes smoothly, Phase 1 human trials on kidneys will begin in 2028-2029. Phase 2-3 in 2031-2033. FDA approval, if all goes well, not before 2035-2037. And for the Israeli market, another 3-5 years after that.
Competition and Collaboration
The Canadian lab is not alone. Groups at Wake Forest, Texas Heart, Mayo Clinic, Kyoto University, and the University of Edinburgh are working in parallel. There will likely be competition, and international collaboration, and ultimately a combined publication from whoever reaches the clinic first.
Who Will Not Be Suitable for Treatment?
Even after the treatment is approved, there are populations who will not be able to receive it. Patients with genetic disorders in cells, patients with active cancer who might develop a tumor from iPSC cells, patients with immediate urgency who do not have 8-10 weeks to wait. It is estimated that about 30-40% of potential kidney patients will not be able to receive the treatment even when it is available.
What Can Be Done in the Meantime?
- If you are on a transplant waiting list, do not pin all your hopes on this technology. It is indeed promising, but will take 10-15 years to reach the clinic. Current treatment, transplant from a donor, remains the best chance in the short and medium term.
- Keep your organs healthy. Kidneys, heart, and liver respond excellently to a healthy lifestyle: a Mediterranean diet, 150 minutes of physical activity per week, quality sleep, and no smoking. These simple actions reduce the chance you will need a transplant by 50-70%.
- Check your kidney function routinely. A creatinine and GFR test once a year after age 50 can identify problems early, when there is still time to stop or slow deterioration.
- If you have early-stage chronic kidney disease, act now. Drugs like SGLT2 inhibitors (empagliflozin) and finerenone have been shown to significantly slow kidney deterioration. A conversation with a nephrologist is critical.
- Consider donating organs. Even if this technology solves the problem in the distant future, today, people die on the waiting list. Marking organ donation on your driver's license or signing a donor card is an act that can save up to 8 people after death.
- Join regenerative research registries in Israel. Sheba Medical Center, Rambam, and Ichilov lead regenerative medicine research. When clinical trials arrive in the country, early registrations will be the best way to join.
- Avoid nephrotoxic drugs if possible. NSAIDs (ibuprofen, naproxen) in high doses and over time, certain antibiotics, and contrast agents in imaging tests, all can damage kidneys, especially if they are already weak.
The Broader Perspective
The story of the organ regeneration lab is not just a story about organs. It marks a profound philosophical shift in how we think about medicine. Until today, medicine was mainly about repair and preservation. When an organ breaks, we try to slow the deterioration, or in the extreme case, replace it with someone else's organ. The regenerative approach opens another possibility: returning the body to a state where it can build a new organ of its own, like a lizard growing a new tail.
This is not just technology, it is a worldview. It says that aging and organ failure are not irreversible processes, but conditions that can be reversed, if we have the right biological tools. And this integrates deeply with the broader trend in anti-aging medicine: more and more, we understand that the human body is a regenerative system, and what is needed is to give it the conditions and tools to do so.
It is also important to note that this is not a solution for every condition. This technology will not replace healthy diet, physical activity, or quality sleep as the foundations of health. It will be an additional tool in the toolbox, not a replacement for existing tools. A person who attends to all the foundations and keeps organs healthy may never need this treatment. A person who does not, will still need a donor or supportive drugs, even if in the future they receive a regenerative organ.
And even if this specific treatment takes another 10-15 years to reach clinics in Israel, it changes how we should think about our future. No longer 'organs that end their lives with the body', but 'organs that have a professional maintenance service and can be renewed'. This is a completely new concept of what it means to be human, and what it means to live a long and healthy life.
It is also important to appreciate the social cost of getting here. Behind every such breakthrough stand decades of basic research, billions of dollars in funding, and thousands of researchers who worked on small pieces of the puzzle. The Canadian lab is not the achievement of one lab, but an accumulation of international work, knowledge sharing, and open publication. It is a reminder of the importance of open science and public funding for basic research.
And finally, the aspect that is not discussed enough: if we succeed in producing organs relatively easily, it will change the entire economy of transplant medicine. A market currently valued at 50 billion dollars a year just on organ transplants, anti-rejection drugs, and dialysis for waiting patients, will undergo a dramatic shift. Drug companies that currently produce immunosuppressants will need to adapt, and hospitals will need to change their business model. This is not just a medical breakthrough, but a broad economic upheaval.
Organs grown in the lab are, therefore, not just a medical novelty. They are a change in the perception of what it means to age, what it means to fail, and what it means to regenerate. It turns regeneration from a dream into a recipe, and medicine from a profession of repair into a profession of rebuilding.
References:
Hospital News - Building the World's First Organ Regeneration Lab
Google News - Original Article


💬 תגובות (0)
היו הראשונים להגיב על המאמר.